
Radiographic Case Review: Pulmonary Metastatic Disease in a Young Australian Cattle Dog

A young Australian Cattle Dog arrived at Sage Veterinary Imaging with fatigue and a palpable head bump, leading to radiographs that revealed an unexpected diagnosis.
Clinical Presentation:
A 4-year-old Australian Cattle Dog was presented with lethargy and a palpable bump on the head. Three-view thoracic radiographs were obtained to evaluate for systemic illness or thoracic pathology.
Radiographic Assessment:

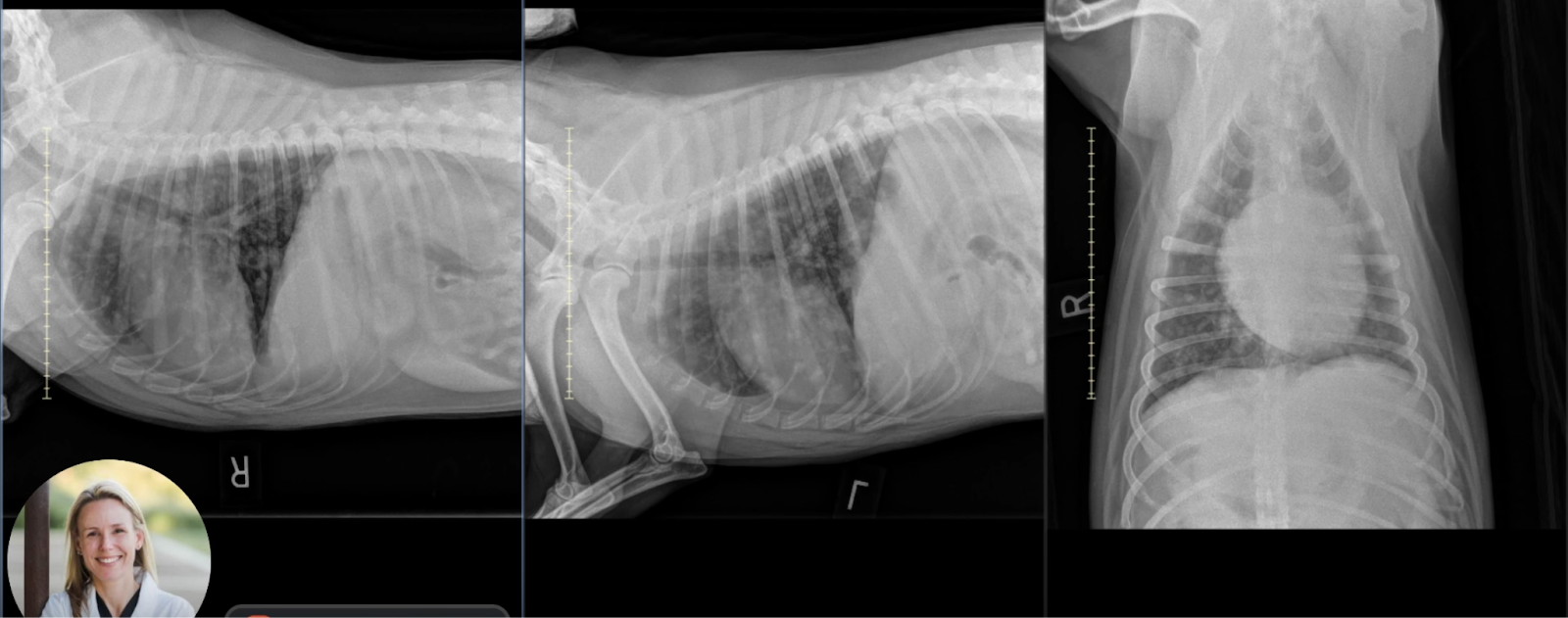
Image 1: Ventrodorsal (VD) View
Cardiovascular and Mediastinal Structures: The caudal vena cava enters the cardiac silhouette normally at the cardiac waist. No left atrial or ventricular enlargement is identified. The trachea is appropriately deviated ventrally, consistent with normal heart size.
Pulmonary Parenchyma: Multiple discrete soft tissue nodules are visible throughout the lung fields, including peripheral regions, confirming that these are parenchymal in origin and not artifacts of summation or vascular overlap.

Image 2: Right Lateral View
Nodular Pattern: Numerous soft tissue opaque nodules are clearly delineated. The largest visible nodule is approximately 1.4 cm in diameter. Distribution is multifocal and involves all lung lobes.
Pleural and Mediastinal Evaluation: No pleural effusion, pneumothorax, or intrathoracic lymphadenopathy is evident. The cardiac silhouette and musculoskeletal margins appear normal.

Image 3: Left Lateral View
Confirmation of Lesions: The soft tissue nodules identified in the right lateral and VD views are reaffirmed, solidifying the diagnosis. Again, there is no effusion or lymph node enlargement.
Interpretation and Differentials:
The radiographic findings are consistent with pulmonary metastatic disease, evidenced by:
Numerous, well-circumscribed soft tissue nodules of varying sizes.
Peripheral and diffuse distribution, helping distinguish them from airway-centered or vascular artifacts.
Dr. Sage reviews the full set of thoracic radiographs in the link below, highlighting how each view contributes to confirming pulmonary metastatic disease.
While metastatic neoplasia is the leading differential, infectious etiologies such as fungal pneumonia—especially blastomycosis—should also be considered. However, this patient lacked a travel history or clinical signs consistent with systemic mycosis.
Ultimately, this dog was diagnosed with a primary neoplasm elsewhere in the body. The radiographic presentation was a typical manifestation of secondary pulmonary involvement.
Educational Notes for Clinical Practice:
Radiographic Technique: Always obtain at least three views (VD or DV, right and left lateral) when assessing for pulmonary nodules. Nodules may only be visible in one view due to summation artifacts and lung inflation variability.
Common Radiographic Signs of Pulmonary Metastases:
Soft tissue nodules of variable size, often well-circumscribed.
Peripheral location helps distinguish true nodules from end-on vessels.
Lack of associated lymphadenopathy or effusion does not rule out metastatic disease.
Differential Diagnosis Tips:
Fungal granulomas (e.g., Blastomyces dermatitidis) may mimic metastases. Consider travel and environmental exposure.
Nodular interstitial patterns from other inflammatory conditions are typically less well defined and may lack peripheral distribution.
Follow-Up Recommendations:
Identify and confirm the primary tumor site via physical exam, additional imaging (abdominal ultrasound, CT, or MRI), or biopsy.
Consider CT for better sensitivity in detecting small or cavitated pulmonary nodules.
Conclusion:
This case illustrates a textbook example of metastatic pulmonary neoplasia, an important consideration even in relatively young dogs presenting with non-specific systemic signs. High-quality thoracic radiographs remain an essential first-line diagnostic tool, guiding the clinician toward further staging and management decisions.
