
Case Study: When “Arthritis” Isn’t the Answer, MRI Reveals the True Cause of Lameness

Meet Ginger
Ginger is a 10-year spayed female Chihuahua who presented with a progressive, non-weight-bearing left forelimb lameness and a slowly enlarging chest mass.
After weeks of treatment without improvement, her case raised an important question: Was this truly arthritis, or something more?
Clinical History
Several features of Ginger’s case indicated that additional diagnostics were needed:
Non-weight-bearing lameness despite appropriate therapy
Lack of response after 12 weeks of multimodal pain management
Presence of neurologic signs (twitching, proprioceptive deficits)
Cervical pain on examination
Suspicion of involvement beyond the joint
These findings raised concern for a neurologic or soft tissue etiology, which cannot be evaluated with radiographs alone.
In our field, this is often the moment where the case shifts away from routine management and toward uncovering what’s truly driving the patient’s pain.
l History
Ginger’s lameness had been present for approximately 12 weeks and had progressed to the point where she was no longer using her left front limb.
She had undergone extensive medical management, including:
Carprofen
Gabapentin
Methocarbamol
A trial of prednisone
Despite these therapies, no meaningful improvement was observed.
Additional clinical findings included:
Intermittent twitching episodes (~once daily)
Proprioceptive deficits in the left forelimb
Pain on palpation of the lower cervical spine
A slowly enlarging chest wall mass
Routine bloodwork remained within normal limits.
Initial Imaging and Diagnostic Limitations

Image 1. Ventrodorsal radiograph of the thorax and forelimbs.

Image 2. Lateral radiograph of the left forelimb.
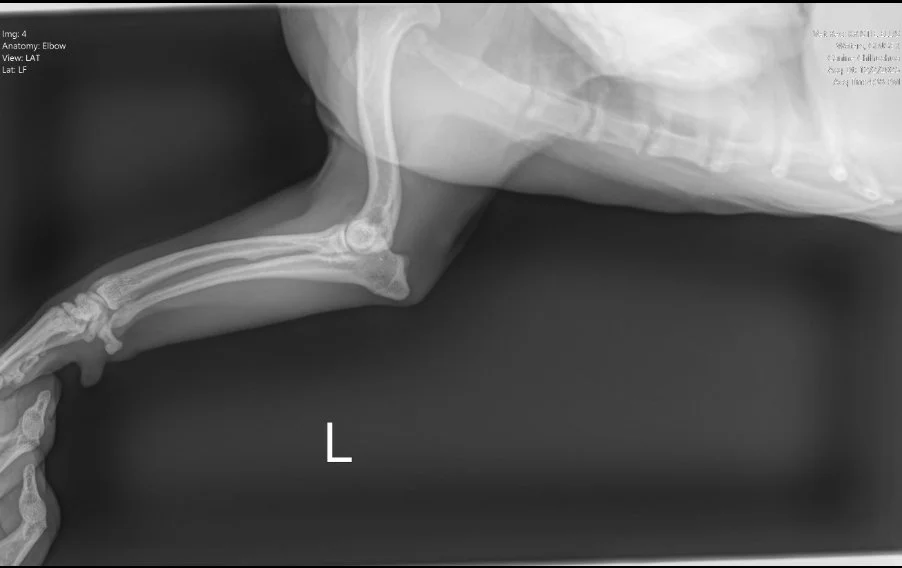
Image 3. Lateral radiograph of the left elbow and antebrachium.
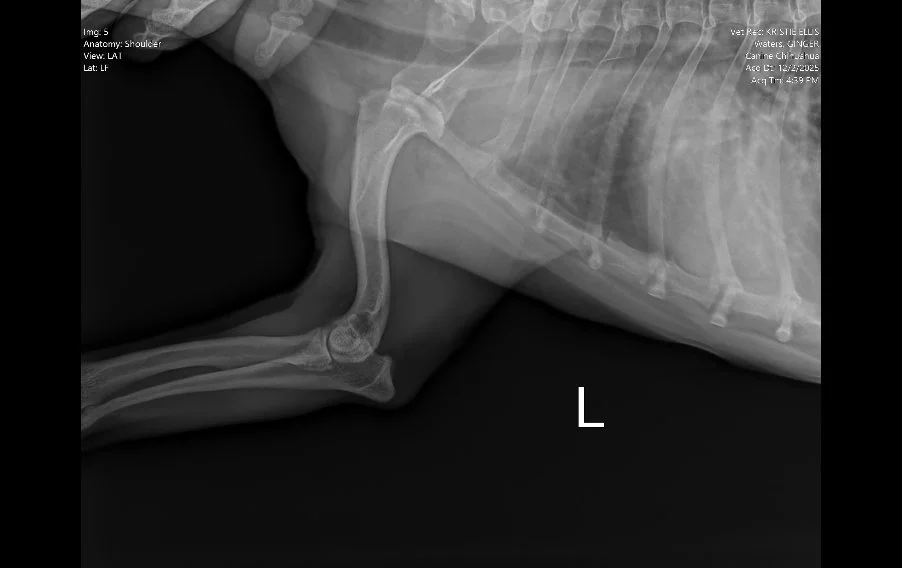
Image 4. Lateral radiograph of the left shoulder.
Radiographs (Images 1–4) of the left forelimb, including the carpus, elbow, and shoulder identified:
Mild degenerative joint disease (arthritis)
Decreased shoulder joint space
No fractures, masses, or bone lysis
Based on these findings, Ginger was treated for osteoarthritis. However, her clinical progression did not match the imaging results.
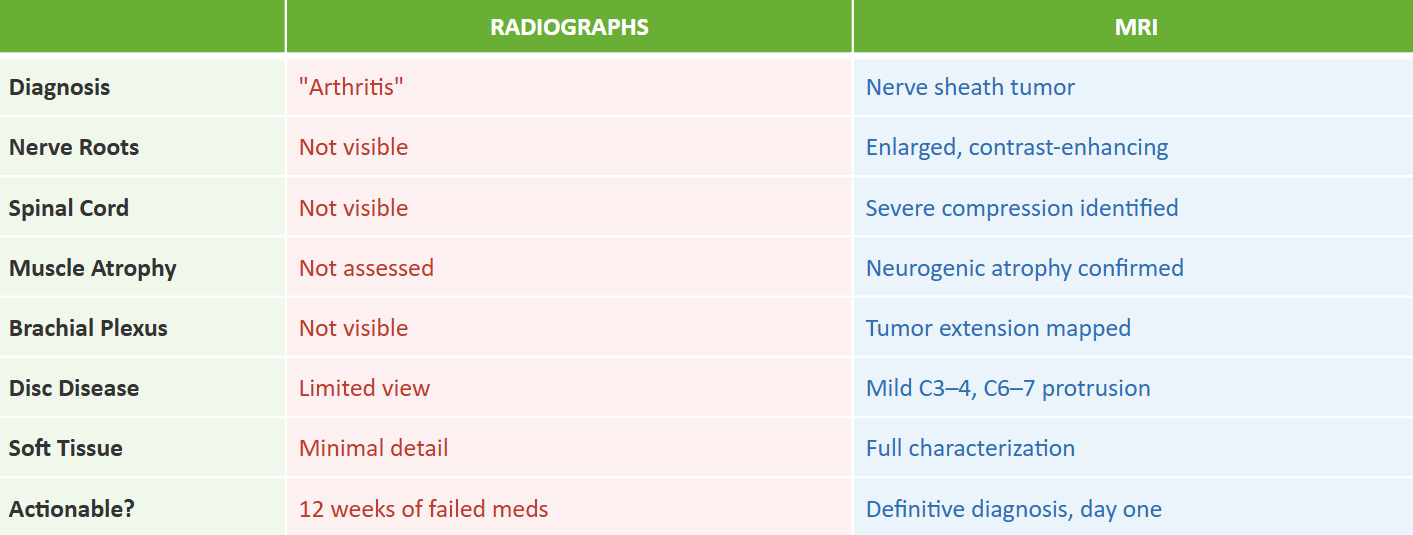
👉 This mismatch is critical. Radiographs are excellent for evaluating bone, but they cannot assess nerve roots, the spinal cord, or most soft tissue structures.
As a result, the true cause of Ginger’s pain remained undetected. This is not uncommon in cases like Ginger’s. Everything can look reassuring on initial testing, but it’s often when we’re brought in that we uncover a deeper, less visible cause for a patient’s pain.
Red Flags That Prompted Advanced Imaging

Several features of Ginger’s case indicated that additional diagnostics were needed:
Non-weight-bearing lameness despite appropriate therapy
Lack of response after 12 weeks of multimodal pain management
Presence of neurologic signs (twitching, proprioceptive deficits)
Cervical pain on examination
Suspicion of involvement beyond the joint
These findings raised concern for a neurologic or soft tissue etiology, which cannot be evaluated with radiographs alone.
In our field, this is often the moment where the case shifts away from routine management and toward uncovering what’s truly driving the patient’s pain.
Why MRI Was Performed
Magnetic Resonance Imaging (MRI) was recommended to evaluate:
The cervical spine and nerve roots
The brachial plexus
The relationship between the mass and surrounding structures
MRI is uniquely capable of detecting nerve pathology, soft tissue masses, and spinal cord compression, making it the gold standard for complex lameness cases involving neurologic signs .
MRI Findings

Image 5. Dorsal post-contrast MRI of the cervical spine and thoracic inlet demonstrating a contrast-enhancing lesion associated with the left-sided C7–T1 nerve roots extending into the brachial plexus.
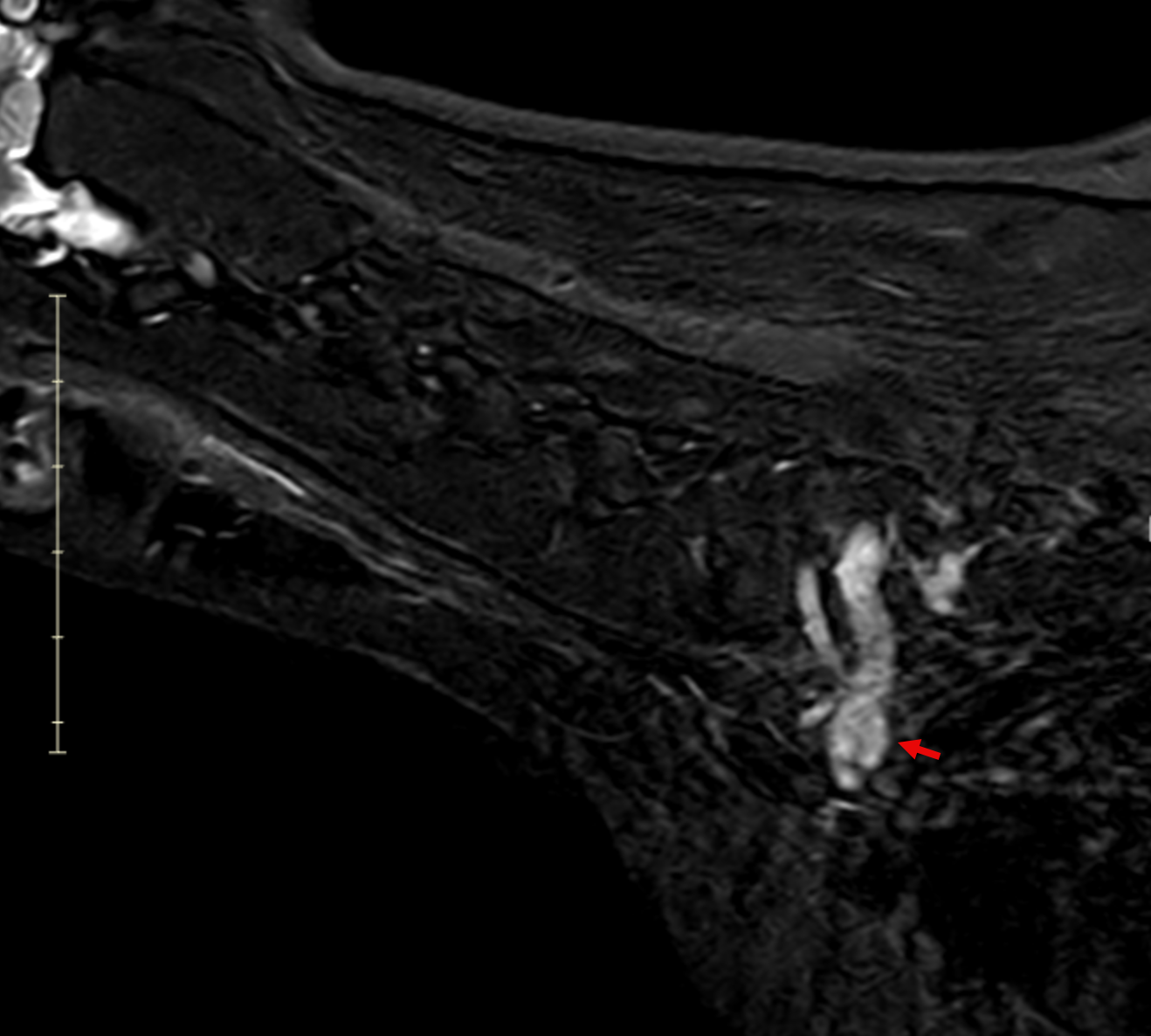
Image 6. Sagittal post-contrast MRI demonstrating a tubular, contrast-enhancing mass extending along the left cervical nerve roots into the brachial plexus, with associated spinal cord compression.
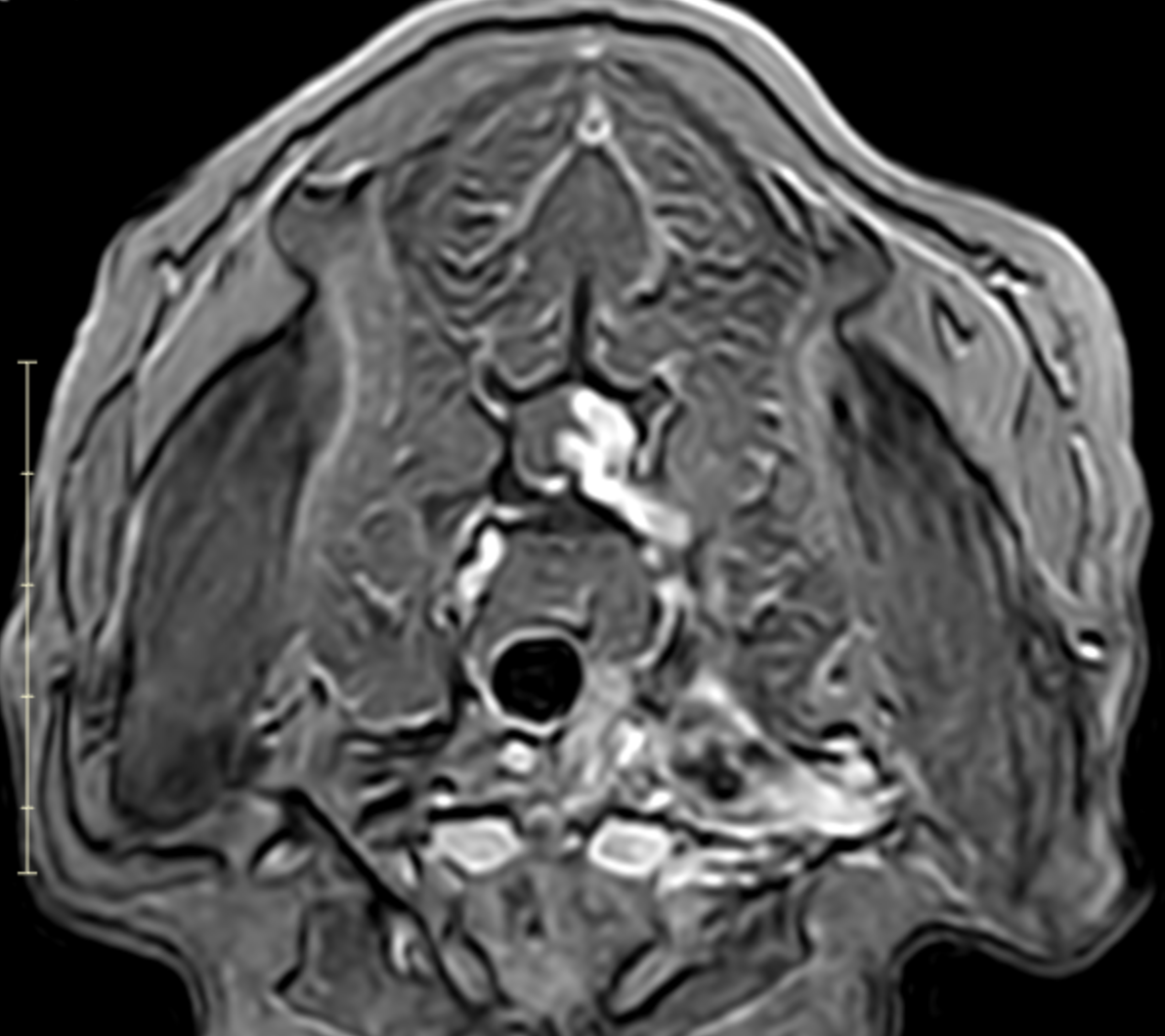
Image 7. Transverse post-contrast MRI showing asymmetric enlargement and contrast enhancement of the left C7–T1 nerve roots with associated spinal cord displacement, consistent with a nerve sheath tumor.
MRI revealed a clinically significant and previously undetected diagnosis (Images 5-7):
Primary Diagnosis: Nerve Sheath Tumor
Contrast-enhancing mass involving the left C7, C8, and T1 nerve roots
Extension from the spinal canal through the intervertebral foramen into the axilla and brachial plexus
Severe spinal cord compression with displacement
Expansion of the C7–T1 neural foramen
Associated neurogenic muscle atrophy of the left forelimb (triceps)
Additional Findings
Mild intervertebral disc protrusions (C3–4 and C6–7), not clinically significant
Evidence of cerebellar cortical degeneration
In other words, what appeared to be a routine lameness case was actually being driven by a much more complex, and previously hidden, neurologic condition.
Interpretation
Ginger’s lameness was not caused by arthritis.
Instead, it was the result of a nerve sheath tumor affecting the brachial plexus, leading to:
Pain originating from the nerve roots
Loss of limb function
Muscle atrophy due to denervation
This explains:
The non-weight-bearing lameness
The lack of response to pain medications
The presence of neurologic deficits
While unexpected, this diagnosis finally explained why Ginger continued to struggle despite weeks of treatment.
Clinical Significance
This case highlights a critical clinical lesson:
When the severity of lameness does not match radiographic findings, the diagnosis is likely incomplete.
MRI allows clinicians to:
Detect neurologic causes of lameness
Identify tumors and soft tissue disease
Avoid prolonged, ineffective treatment
Earlier advanced imaging could have shortened Ginger’s diagnostic journey and provided answers sooner.
Client Perspective
Ginger’s family had been searching for answers for months.
“⭐⭐⭐⭐⭐ - After 12 weeks of trying different medications, we finally got an MRI and a diagnosis. Though it wasn’t the news we hoped for, we finally understand what’s going on and what steps to take next. We’re so grateful to have answers.”
Key Takeaways
Not all lameness is orthopedic, neurologic causes must be considered
Radiographs have limitations, particularly for soft tissue and nerve disease
Failure to respond to treatment is a diagnostic clue, not just a treatment problem
MRI is the gold standard when neurologic involvement is suspected
Summary
Ginger presented with chronic, progressive lameness that was initially attributed to arthritis based on radiographs. However, MRI revealed a nerve sheath tumor involving the cervical nerve roots and brachial plexus, completely changing our understanding of her condition and the path forward.
This case is a powerful reminder that when imaging findings don’t fully align with what we’re seeing clinically, it’s worth taking a deeper look.