
Radiographic Case Review: Linear Foreign Body Obstruction in a Young DSH Cat

A young domestic shorthair cat presented for acute vomiting and dehydration after suspected ingestion of yarn.
Clinical Presentation:
A 1-year-old male neutered domestic short hair cat presented for acute vomiting—reported approximately 16 times over 24 hours—and inability to retain food or water. The vomitus became blood-tinged, and the cat was known to play with yarn. On examination, the abdomen was soft but uncomfortable, and the patient was moderately dehydrated.
Radiographic Assessment:

Image 1: Left Lateral View
Stomach: Mildly gas and fluid-filled, slightly more than typical in a feline stomach.
Pylorus: Appears normally gas-filled without visible foreign material, suggesting that any anchor point is distal to the stomach.
Small Intestine: Extensive plication throughout the abdominal cavity with serpentine and bunching patterns, indicating a linear foreign body obstruction (LFBO).
Colon: Moderately filled with formed fecal material; although this may seem inconsistent with obstruction, it is not uncommon in feline LFBO cases due to gastrocolic reflexes.

Image 2: Right Lateral View
Small Intestine: Reaffirms severe plication with fragmented intraluminal gas and stacked loop crowding. The pattern of angular, closely apposed loops is classic for LFBO.
Colon and Rectum: Contain some fecal content but no obstruction visible at this level.

Image 3: Ventrodorsal (VD) View
Loop Orientation: Plicated loops are centrally displaced, often forming radiating, serpentine patterns.
No foreign body is directly visualized, but the overall pattern confirms functional obstruction.
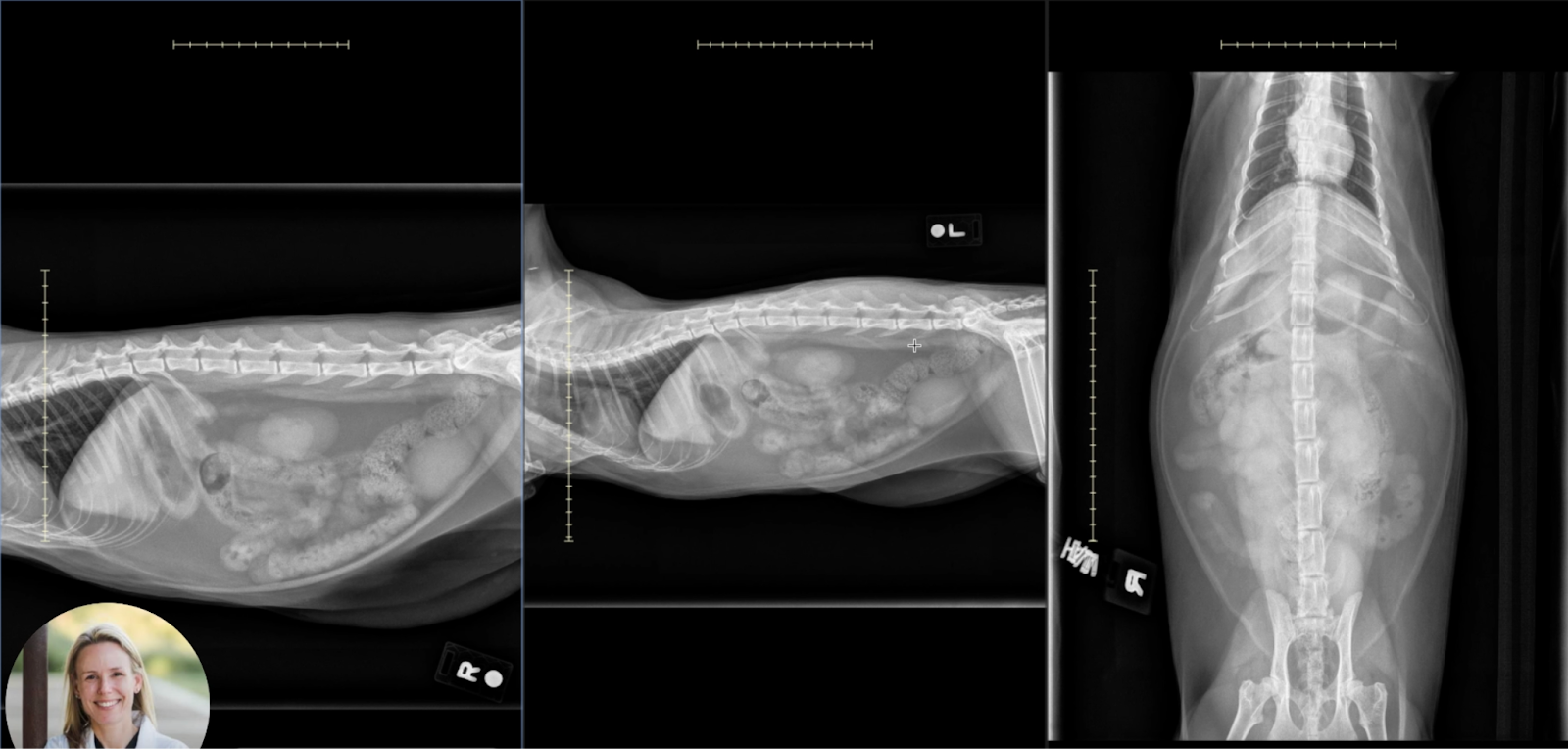
Image 4: Composite Overview
This comparison of orthogonal views highlights:
Global plication with accordion-like narrowing of the small intestines.
Fragmentation of gas bubbles, discontinuous lucency, and poor distinction between adjacent loops.
Interpretation and Differentials:
Radiographic findings are consistent with:
Linear foreign body obstruction (LFBO) with plication of nearly the entire small intestine.
No evidence of bowel perforation or free peritoneal gas.
The suspected linear object (e.g., yarn) is anchored distal to the pylorus, allowing gas-filled loops proximal and distal to the anchor point.
Differentials considered but deemed less likely:
Mechanical obstruction from a discrete object (would typically cause segmental dilation without plication).
Functional ileus (would not show this level of structured plication or gas fragmentation).
Enteritis (more diffuse pattern, no bunching).
Educational Notes for Clinical Practice:
Classic Radiographic Signs of LFBO in Cats:
Plication of small intestine with overlapping, bunched loops.
Fragmented intraluminal gas or “beaded” gas pattern.
Serpentine loop morphology in multiple planes.
Gastric and colonic evacuation may persist due to reflex emptying, not ruling out obstruction.
Differences from Canine LFBO:
Cats often present more uniformly plicated small intestines.
Foreign material (e.g., thread, yarn) is less radio-opaque than dog toys, requiring interpretation based on secondary signs.
Peristalsis in cats may persist longer, which can delay clinical recognition.
Follow-Up Recommendations:
Ultrasound for foreign body confirmation, gastric/intestinal wall viability, and perforation.
Surgical intervention is urgent when clinical signs and radiographic plication are present.
Pre-operative management: IV fluids, electrolyte correction, and pain control.
Conclusion:
This case illustrates a classic feline linear foreign body obstruction, with textbook examples of plication, serpentine intestinal loops, and fragmented gas. Despite the presence of feces in the colon, the severity and uniformity of small intestinal plication warrants immediate surgical evaluation.
In feline practice, this is a critical case to recognize early, even when foreign material is radiographically occult.
